
Primary osteochondritis of the hip or LEGG PERTHES disease and
CALVE or coxa -plana is a condition frequent, affecting mainly the boy between 3 and 12 years old, she occupies the 2nd place of orthopedic alterations after luxating hip disease.
What is a PHO ?
It is a disease of all the upper end of the femur or predominantly partial necrosis of the upper epiphysis of the femur without doubt of vascular origin.
Reminders:
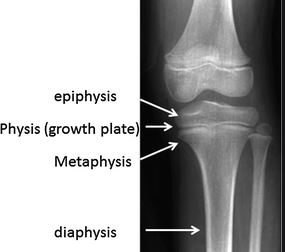
DIAPHYSIS: middle part of a long bone EPIPHYSIS: swollen end of long bones METAPHYSIS: intermediate part between diaphysis and epiphysis. APOPHYSIS: growth of the surface a bone sometimes serving as a bone surface to a joint.
Pathophysiology of the PHO
The vascular interruption can be explained by minimal trauma or
repeated (common in boys) and precarious position of the vessels
upper epiphyseal. The duration of ischemia will determine more
or less diffuse. Altered cartilage are never totally destroyed and
the repair effort is constant.
The growth harmony of the extremity femoral superior is ruptured, the cervix will be: brief, widened transversely and circumferentially, (hypertrophy and varus by the trochanter). The acetabulum model on this deformed head. It exists reciprocal action between the head femoral and acetabulum until the end of the growth (interest of osteotomies pelvic and femoral).
Exploration interrogation
In 80% of cases, it is a boy between 3 and 12 years old. The first symptoms are relatively late and do not appear only a few months after the actual start of disease. It could be :

-pain, hip, thigh, or knee occurring at the fatigue or exertion (prolonged walking).
-a lameness occurring when tired and decreasing at rest, analgesic type.
-sometimes a hip blockage with functional impotence: impossibility of support on the lower limb.
Analytical and functional clinical reports
The clinical examination looks for a joint limitation, evident in case of
blocking, much more difficult to put prominently in other cases.
It is careful examination on a hard plane who will find by comparison to the side opposite:
1. a limitation of internal rotation
2. a limitation of abduction
3. a limitation of hyperextension.
The vicious attitude will be addictive, external rotation and bending. It exists sometimes an amyotrophy of the thigh and quadriceps testifying to seniority lesions.
General and paraclinical report
Radiographic examination is essential, it must include a snapshot of the pelvis face, and a profile of each hip or bilateral anteversion. The signs of start should be searched with Warning :
- image in nail stroke on the part superior of the cephalic nucleus
- flattening and condensation of the nucleus cephalic
- infero-internal enlargement of interlining
- central condensation of the nucleus -metaphyseal reaction with geode and enlargement of the cervix.
At the state phase: whitish appearance sequestration with geodes and images of bone resorption. The phase of restoration results in a
remineralization, with peripheral border encompassing the respected sectors. At the sequelae phase: this is the COXA-PLANA which should be avoided at all price. Two criteria are important:
THE EPIPHYSIS INDEX (max. of the epiphysis / max. epiphysis)
must be greater than 60.
THE CONCENTRICITY OF THE CORE CEPHALIC IN RELATION TO ACETABULAR. Head and cup should register on concentric circles spaced 2 mm apart. A good hip does must not have a loss of concentricity greater than 2 mm.
We will distinguish:
Round heads: having lost their height, but whose line spacing articular will remain parallel to the acetabulum.
Flattened heads: prognostic coxa plana strict.
Classification
A classification of damage in 4 groups was proposed by Catterall.
This classification is based on 2 hypotheses:
1. the attack is all the more serious as the necrosis is more extensive
2. The extent of the ischemic attack is determined from the start, it is superimposed on vascular topography it is recognizable a few months after clinical onset.
GROUP 1:
The lesions are diffuse and slight on the
cephalic nucleus, the marital plate
is not affected. The attack is isolated at
anterior sector.
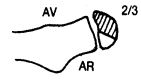
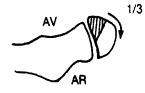
GROUP 2:
The infringement concerns half or 2/3
anterior of the nucleus there persists a sector
living posterior providing support.
GROUP 3:
Anteroposterior necrosis is
inconstant. The extension to the plate marital causes disorders
metaphyseal steadily.
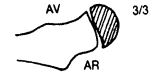
GROUP 4:
Total damage to the nucleus
epiphyseal, and very important at the level
of the marital plate. The metaphysis
bone is still severely damaged.
PROGNOSIS
GROUP 1:
Always spontaneously good, it’s young children (5 years).
GROUP 2:
The living posterior sector provides care and support. We can hope for a good quality distribution.
GROUP 3:
Evolution depends on the distribution of forces and the acetabular mold.
GROUP 4:
The joint can maintain a roundness and congruence, the aftereffects are sometimes less important and less earlier than those in group 3.
The prognosis depends on the degree of bone maturation. The older the bone age will be advanced, plus the O.P .H. will be severe from
has less potential for remodeling.
CONCLUSION
Primary osteochondritis of the hip is a complex disease whose repair is unpredictable. The evolution is very long, risking does prolonged immobilization: amyotrophy and joint stiffness. The rehabilitation will have to take into account school requirements, state child’s psychological, and parental cooperation.